

A Child and a Ventilator
Kidnapping at Children's Hospital?

The Truth and Freedom movement brings me into contact with families from all walks of life. Here is a case that should concern families worldwide.
Baby T is a 16 month old child who wasn’t born with the maintenance free body that most other children have. He has VACTERL, a Double Outlet Right Ventricle and a TRAF 7 gene anomaly. His body is so unique that there is no expert on Baby T’s situation. What brought Baby T’s parents to me?
Baby T’s medical team had called upon a social worker to remove him from his parents care.
Why?
Baby T’s parents have successfully raised 3 other children to ages 3, 7 and 9 years of age without issue. What is going on with their 4th child that suddenly needs a social worker?
After talking with the parents, and digging through Baby T’s medical records, what I saw were occasional differences of medical opinion between parents and pediatricians. In the case of someone like Baby T, no one actually knows what is best. He is such a unique case that the best the Children’s hospital pediatricians can do is make educated guesses — the combination of anomalies Baby T has is that rare. So if no one actually knows what the “right” medical answer is, why would any doctor have anything against reasonable medical requests from the parents?
Then I saw something that hit particularly close to my heart as an ER doctor with experience in critical care.
Ventilators (again?)
In the emergency room, ventilators are a cornerstone of critical care. If the patient doesn’t have enough oxygen, everything else eventually fails. The deadly consequences of misusing this life saving invention, is described in one of my previous articles.

In my critical care training, it was a daily responsibility to check ICU patients every day to see if they could be taken off their mechanical ventilatior. The longer a patient receives ventilation, the higher the likelihood of Ventilator Associated Pneumonia (VAP). Typically for ICU patients, that meant decreasing sedation to see if the patient could wake up enough to breathe on their own. Modern ventilators keep record of patients breathing on their own or attempting to do so with “triggered” breaths. When a ventilator alarm repeatedly indicates that the patient is breathing over the ventilator, and if oxygen levels are stable, the signs are there that a patient is ready to start breathing on their own.
What was Baby T’s situation?
He started breathing on his own.
This started a conflict between Baby T’s parents and his “Children’s Hospital” doctors over giving Baby T more chances to breathe without a ventilator:
Baby T’s parents had requested for months that his ventilator be gradually reduced to help him to learn to breathe on his own, and possibly help with his tracheomalacia.
Tracheomalacia is the condition where the rings of cartilage that keep the airways open are too weak to keep the trachea and bronchi open during the negative pressure created when we breathe in.
Imagine trying to draw air in through a paper straw that is so wet it collapses with suction because it lacks the stiffness to stay open. That is a similar situation to what occurs in tracheomalacia.
As a result positive pressure from a ventilator is used to keep the airways open.
About midway through medical school, almost 20 years ago, I learned that chondrocytes (the cells that make up cartilage) can be stimulated to grow and mature with mechanical pressure.
As of April 2020, nothing has changed. Our knowledge of cartilage metabolism still teaches that mechanical stimulation is essential for growth and maturation. So the principle that pressure might help improve the health of cartilage is nothing new. (Certainly not new for the past 20 years.)
Wouldn’t lowering the air pressures on the ventilator allow for more mechanical pressure on the tracheal cartilage, stimulating it to grow and strengthen?
Why would the pediatricians be so resistant to reducing the ventilator?
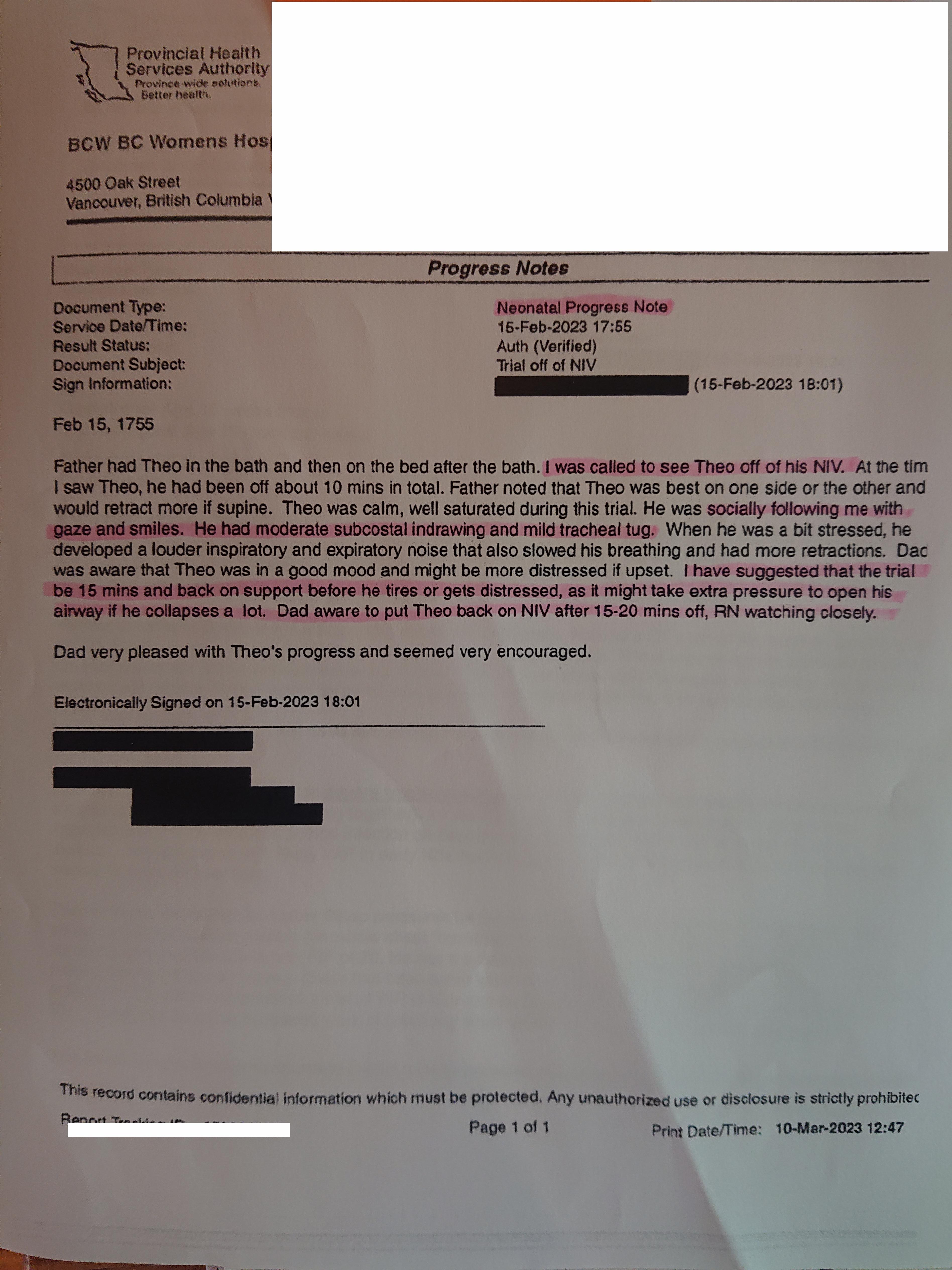
On February 15th, 2023, the Father observed Baby T successfully breathing without a ventilator after a bath. (The ventilator in these medical records is called an “NIV”— Non-Invasive Ventilation).
This is the note written by the first doctor who examined Baby T breathing without the ventilator.
{kind=link}
I might have written a similar note if a nurse called me to reassess a baby who was found to be breathing adequately without a ventilator when he previously needed one.
Similar to the ICU, signs that patients are able to breathe without mechanical assistance are a welcome improvement on the path to recovery. It would typically be followed by more steps to reduce the ventilator till the patient can fully breathe independently.
This doctor suggested 15 minutes off the ventilator, and then wrote “Dad aware to put (Baby T) back on NIV (non-invasive ventilator) after 15-20 mins off…”
All is good right?
However, then the STORY CHANGED.
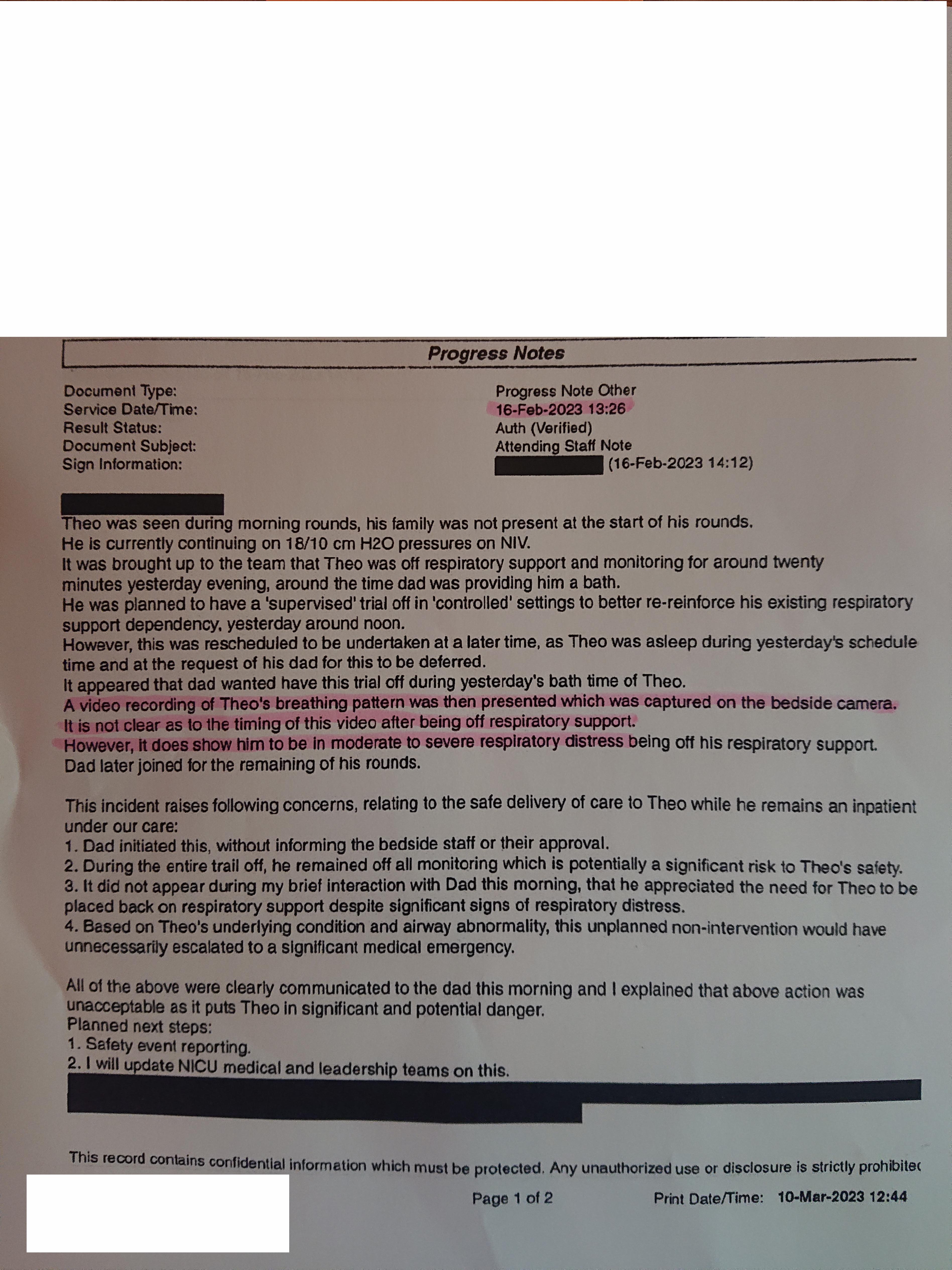
Here is what the “Attending Staff” wrote the next day:
{kind=link}
In the hospital world, “Attending Staff” is a bit “Higher Up” than the doctor on call who was called to assess Baby T at about 1755 on February 15th, 2023.
What !!! ???
How does the description of Baby T’s breathing go from:
“Moderate Subcostal Indrawing” and “Mild Tracheal Tug” from the first pediatrician to:
An “Attending Staff” viewing a video of Baby T and a day later writing:
“However, it does show him to be in moderate to severe respiratory distress being off his respiratory support.
Mild tracheal tug which I’ve seen thousands of times in the ER, is very different from “moderate to severe respiratory distress”. It makes me wonder if this “Attending Staff” actually knows what constitutes a medical emergency.
Maybe the nurses note can help?
(The trilogy headpiece she mentions in her note is the nasal mask for a BiPap ventilatory assistance machine.)
This “Nursing Narrative Note” is 3 days after the fact on February 18th. So between February 15th when Baby T was breathing on his own after a bath, and February 18th 15:34, there may have been some “influence” on our nurse’s “recollection” of events.
What kind of “Influence”?
The “Attending Staff” pediatrician’s note from February 16th concluded, “…this unplanned non-intervention would have unnecessarily escalated to a significant medical emergency.”
Was the nurse “advised” that the medical team decided something “terrible happened” before she wrote her note on Baby T’s chart 3 days later?
A day after Baby T was caught on video BREATHING ON HIS OWN “WITH SMILES” (according to the doctor who actually examined him that day);
THE MEDICAL “TEAM” CONCLUDED that him breathing without a machine:
“…would have unnecessarily escalated to a significant medical emergency” ?
Are these people even doctors?

If you read the above carefully, there even seems to be an implicit threat against the father.
(There might even be an EXPLICIT threat against the father or family — I cannot tell because something was redacted in black before these records were given to the parents.)
What should be celebration about medical progress for a baby with multiple rare medical conditions has suddenly turned into an attack on the Father?
What is wrong with this medical “TEAM”?
Getting back to our nurses note written 3 days after the fact:
(Considering there might be significant influence from “medical and leadership teams” on how our nurse “remembers” the events of February 15th, 2023.)
Our nurse stated:
There was “Moderate work of breathing.”
“Subcostal, Substernal, and tracheal tug noted.”
“Writer (the nurse) took video of (Baby T) off support as previously discussed with team…”
The Nurse has a video of Baby T breathing without a ventilator on February 15th?

Where is this video? Is it on the medical record?
Why did the doctors not give the parents a copy of this February 15th video OF THEIR OWN BABY?
The nurse goes on to say that:
“Dad kept (Baby T) off for at least 30 minutes total”, and
“Work of breathing was more moderate compared to on NIV (ventilator) support. (Baby T) was happy throughout the trial off and was smiling and engaged.”:
What does “more moderate” mean? (I don’t know and I’m a doctor.)
However, from a medical standpoint, I do know that “(Baby T) was happy throughout the trial off, and was smiling and engaged.” IS NOT “A SIGN OF MODERATE TO SEVERE RESPIRATORY DISTRESS”!
(Just who is this Attending Staff pediatrician to make this claim — without actually being there while the patient was off the ventilator? I wish we knew, but his name is redacted.)
You decide… “Severe Respiratory Distress” or “smiling and engaged”

This is the only video the parents have of Baby T breathing without the assistance of a machine. They were forbidden by social workers to take videos of their own baby to post on social media. This video was from May 2nd, a week before Baby T went for surgery to install a Tracheostomy.
A Tracheostomy is a ventilation port in the neck that is installed when a patient’s condition is expected to need long term ventilation for many months or years.
How can the pediatricians conclude that Baby T needs surgery for long term ventilation if they haven’t even given Baby T a chance to breathe on his own?
(No one is an expert on the comination of conditions that Baby T has.)
In fact, if anything it looks like the “staff” pediatrician was willing to lie about Baby T in order to PREVENT any further attempts to reduce Baby T’s medical dependence.
(As an aside, the parents never gave consent for the Tracheostomy surgery. Social workers with no medical training took over medical decision making from the parents on April 19th 2023.)
Who requested that medically unqualified Social Workers take over medical decisions for Baby T?
Was it the doctors who asked social workers to take away the parents rights?
Did the doctors do this because the parents were trying to get Baby T breathing on his own? (Without a ventilator?)
I don’t know.
But it is very suspicious, and there is a discrepancy between what I expected doctors to do and what the Canadian pediatricians at Childrens Hospital actually did (and are continuing to do).
For more about discrepancy analysis:
Medical decisions and Social Workers
(My first experience with social workers)1
Have a listen to this conversation between Baby T’s social worker and his father.
(I apologize for the length of the conversation, but I included it in its entirety so people can see the big picture.)
Does this social worker sound like she cares about Baby T’s health?
Is this social worker medically competent?
(if not, then why is she making the medical decisions?)
If you think the “Attending Staff” pediatrician’s medical note above is dishonest and suspicious, have a look at this social worker’s description of the exact same event:
If there ever was something that you could call a lie…
Fast forward to today.
On Friday August 18th, the social worker stopped Baby T from having any visitation from his MOTHER. The alleged reason was because the mother brought in an “unauthorized visitor” (me) on August 10th, 2023. When I visited Baby T, I saw a happy active baby being ventilated via a tracheostomy. I offered his pediatricians a detailed medical explanation why the parental requests to wean Baby T’s mechanical ventilator was MEDICALLY REASONABLE.
I also explained the medical reasons why allowing Baby T to have have longer breaks between tube feeds might be beneficial in reducing the load on his heart. I heard his pediatricians complain that Baby T was not gaining weight as well as they expected, but the only problem they considered was that maybe Baby T was working too hard to breathe. Slow growth could be natural for Baby T’s body, or a side effect of brain compression from his unmanaged cranial synostosis2. while the pediatrician in training considered the medical validity of the parents wishes, the “staff pediatrician” was an entirely different piece of work (but that’s a story for another day). The end result is a medically unqualified social worker has banned Baby T’s mother from all visitation and contact.
Is this social worker doing things to HELP Baby T or HARM him?
YOU DECIDE.
My first memorable ER incident with a social worker happened years ago when I was working in a large suburban ER (which was for a brief time the largest Emergency Room in Canada).
A terminal cancer patient was taken from her home by police at the instruction of a social worker and brought in to the Emergency Department against her will. Before I even started seeing this patient, a social worker approached me and told me that I “Had to Admit” the patient. She claimed the patient was a victim of elder abuse from her son, because she was not filling her prescriptions for NARCOTICS and was taking marajuana products instead for her Terminal Cancer! I told her politely that I would evaluate the patient first and go from there, and she stormed off furious that I did not immediately take her “Social Work ORDER!”
When I walked in the patient’s room, I saw a middle aged son sitting quietly at the bedside, and a 70 ish mother who was high. She had metastatic cancer charted in her medical records, and there was one metastasis on her neck that looked either inflamed or infected. The social worker returned as I was evaluating the patient and repeated again that it was not up to me, that I had to ADMIT the patient to hospital. I told her, the patient’s only medical problem is metastatic cancer, and the fact that she is high does not mean she needs to take up a hospital bed or an acute ER bed. If she decides when sober that she wants to go home, she has the right to do what she wants.
This social worker insisted that this terminal cancer patient couldn’t make her own decisions, and that she was ordering me to put her in hospital against her will. I told her I would bring the patient around from her state of being high, and if she is competent when she is no longer high, I will let her make her own medical decisions.
I gave her fluids until she was no longer high, and then asked her if she comprehended her medical situation, and what she would like to do. She said she wanted to go home. I offered her IV antibiotics for her inflamed or infected cancerous metastasis and if it did not resolve the redness, she could discontinue it any time during her daily reassessments in hospital.
Despite this concilliation that a doctor would be reevaluating her daily to make sure there’s no signs of elder abuse while treating her metastasis, this social worker filed a complaint about me regardless.
Did this social worker ever get disciplined for abusing a terminal cancer patient by dragging her out of her home with police because she was high? (I don’t know)
Craniosynostosis is when the bone plates of the skull are prematurely fused preventing the brain from growing as a baby matures.
To what end does the medical industry need to separate a child from his parents? Force medical interventions that are expensive and most possibly unnecessary in our universal Healthcare program? Are they experimenting? Are they abusing a child and his parents for power? Why would a social worker seek out this kind of adversity when none existed until the social workers appearance, again a miss use of limited resources? Are hospitals incentivesed to keep experimental procedures going? Don't we have enough to deal with and fund without searching out situations that are questionable, at best.
Loving caring parents should never have their wishes ignored and never, ever be banished from a child's life. The social worker and chief physician are heartless cruel robots acting for the machine.
Jesus ! how many time did the social worker repeat the phrases, 'Be careful' and 'I know'. That's quite threatening like the abuse of power. V competent practice (being sarcastic here).
Tho I am not entirely familiar with the Canada's Child welfare system (it looks like the social workers are given the legislative power to remove the child without a court order or without an assistance from the police, which is different from the UK system.), I used to work with Canadian SWs in the UK and would assume the ground work (concept ) for the child care SW is more or less the same. From the social aspect of the situation, firstly I would like to see the risk assessment made by the social worker. (Must be a written record)
What (potential) risks did the mother and subsequently the 'unauthorised visitor' present ? Particularly I am concerned for the child's attachment to the mother being abruptly halted. (No offence to the father!) Was the (potential ) risk great enough to severe the contact with the mother alone? How did the SW decide it was not in the best interest of the child? I looked up BC's children's hospital site and it explains the role of SW. No ref to the SW 's involvement in medical decision making. On the contrary, their primary role is crisis intervention and familial support. (That's how it should be)
Somebody in the hospital has to make a referral to the SW dept. Who made that referral?
I am not getting the impression the social worker is playing an advocacy role here for the child either. She is only delivering the message from the hospital mgt.
And the father was right in asking for family counselling.
I bet it was a risk (threat) posed to the establishment (hospital), not to the child. ( Puzzling medical procedures seem to be going on and subsequent cover ups. Otherwise, no 'unauthorised visitor' should pose a threat if they are competent.
That can only explain the SW's incompetent intervention.
I used to think Canadian SWs are well trained. But obviously their standard must be going down the hill then.
Thanks Justin & friends!